Question: How do I decide when to discontinue services for a patient/client who has been receiving it for a long time?
This is probably the 2nd most common question we get, just behind “How do I determine when the child should receive services?” This is not surprising, as the question of when our services are needed and not needed is complicated and requires sound clinical reasoning.
If you discontinue services too soon, you risk the client not reaching their potential, or losing their functional gain. If you continue providing services when it is no longer necessary, you are overusing valuable resources, yours and the client’s, that are better spent elsewhere (e.g., your time and skills for another client who definitely needs it; your client’s time and experiences being with peers).
In an attempt to come up with a more universal answer, we will refer to our professional association’s guidance for discontinuing services. However, make sure to consult your state and local regulations and or policies for additional guidance.
-
-
- AOTA’s OT Practice Framework – 4 (2020) states “Discontinuation of care occurs when the client has met short- and long-term goals or chooses to discontinue receiving services”, p. 32.
- ASHA’s Admission/Discharge Criteria in Speech-Language Pathology Guidelines states that “Patient/client discharge from treatment ideally occurs when the individual, family, or designated guardian, and speech-language pathologist as a team conclude that the communication or feeding and swallowing disorder is remediated or when compensatory strategies are successfully established”. It also states that discontinuation is appropriate if “8. The individual is unwilling to participate in treatment; treatment attendance has been inconsistent or poor, and efforts to address these factors have not been successful. 9. The individual, family, and/or guardian requests to be discharged or requests continuation of services with another provider.”From https://www.asha.org/policy/gl2004-00046/#sec1.4
- APTA’s Guide to PT Practice (2014) provides the following criteria for discharge:
- When the goals or outcomes for the individual have been achieved,
- When the individual is unable to continue to progress toward goals,
- When the individual chooses to conclude care, or
- When the physical therapist determines that the individual will no longer benefit from continued PT
-
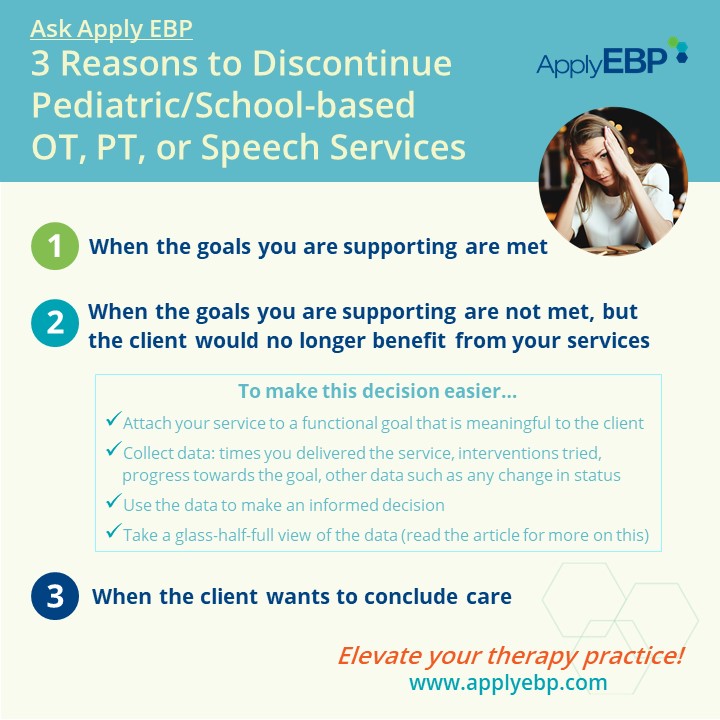
So based on these, this article will discuss 3 reasons to discontinue pediatric/school-based services:
-
-
- When the goals you are supporting are met
- When the goals you are supporting are not met, but the client would no longer benefit from your services
- When the client wants to conclude care
-
Also, note that in this article, I will use the term “team” to refer to different types of teams depending on your setting (i.e., IEP team in the school setting, medical team in the clinic, home care team for the home setting), with emphasis that the client is part of that team.
When the Goals You Are Supporting Are Met!
Meeting goals is the ideal outcome, making the decision to discontinue services easier. Assuming the team created participation-/occupation-based goals, our clients is now able to participate with peers, family, or others, in activities that are meaningful to them. Present this information as a celebration…that’s why I prefer the more positive term, graduation from services! The client has succeeded and no longer needs your services to continue with this success.
By the way, the focus on achieving functional goals is further supported by ASHA’s statement that “…disorder is remediated or compensatory strategies are successfully established.” This reinforces that our role is not necessarily to fix impairments, but rather to help them succeed in real-life activities, such as communication, mobility, ADL, etc. We can achieve this with compensatory strategies, or alternative ways of performance that suit our client.
But something to note here is that achievement of a goal only means our services are no longer needed for that particular goal:
-
-
- If the team establishes another goal (e.g., a higher level of the achieved goal, or an entirely different goal), your services may continue to be needed for that newly-established goal.
- It is also possible that our services may not be needed now, but maybe needed at a future time when there is a new goal that requires our expert interventions. This is especially true for our clients with lifelong disabilities who may need us for multiple episodes of care (e.g., to achieve classroom goals in elementary school, then again later for transition goals in high school).
-
This way, I like to think of our services as always attached to a goal! This is even more important in school-based practice when providing services under IDEA. OT, PT and Speech are related services, and therefore, should “relate” back to the child’s IEP goal(s). This is why in a study of school-based practice guidelines, we stressed that the “team establishes the student’s IEP goals prior to determining whether PT is needed to address any of the goals.” (Vialu and Doyle, 2017). This requires more conversation for another article…
When the goals you are supporting are not met, but the client would no longer benefit from your services
This is the trickier situation. Who wants to accept being unsuccessful in helping their client achieve their goals? I’ll get to the half-glass-full perspective on this later, but for now let me say that for any decision-making, data is your friend! This way, instead of being perceived as making “personal” subjective decisions, you are seen as making decisions objectively.
Data you need to gather:
-
-
- Multiple times you delivered services
- Multiple evidence-informed interventions within your expertise that have been tried
- Fidelity or adherence to the interventions
- Progress (or lack of) towards the functional goal.
- Other relevant data, such as a change in health status, classroom setting, home situation, etc.
-
As I said, data is your friend. If you have all of these data, it will be easier for you to write a report and present your findings and recommendations with confidence!
Arguments to Support Continuing Services
You may support continuation of services if this data tells you that
-
-
- Not enough attempts have been made yet to effect change, especially as it relates to the intervention you are implementing
- The child seems to be improving, and just needs more time
- Perhaps, you need to try a different intervention that has been shown to work for this particular case
- Not enough carryover is happening, so you need to change your strategy to allow skill practice outside of your “sessions”
- A change in status means your services are needed (even more so) now
-
Arguments to Support Discontinuing Services
If the data shows that despite multiple delivery of multiple interventions, the client was unable to achieve the goal, then your services may not be needed. If the client has been receiving the services for a long time, this would mean that you would have several data points to support your conclusion. When presenting this difficult information, try using graphs, or charts to show the above data.
Alternatively, your data may show that due to a change in status, the client/team’s priorities have changed and that the goal is no longer relevant. This may happen when the client’s needs are now being met due to a change in the classroom setting or services. Or that the client’s priorities changed due to a medical regression.
Now, my glass-half-full perspective on this: the data you presented leads to informed decision-making! For example,
-
-
- The team may decide to try a different intervention from another team member that may benefit the client,
- The team may decide to reassess the goal and calibrate it to something that may be more achievable while remaining meaningful, or
- The team may come up with entirely new goals that are more relevant to the client’s change in status
-
So, don’t look at it as a defeat, but a learning process…and present the data as such! Finally, remember multiple episodes of care? Your service may not be needed now, but it may be needed at a future time when your services can benefit your client best.
When the Client Wants to Conclude Care
The trio of the AOTA/APTA/ASHA adds that the client can also decide to conclude their own care. In pediatric practice, the client may refer to the child and/or the parent/caregiver.
This makes a lot of sense, especially when viewed through the lens of self-determination. There are 3 critical elements to self-determination: Autonomy, Competence, and Relatedness. When these 3 are supported, the client is more likely to be motivated to act towards a goal.
So, we need to respect our client’s autonomy, including their ability to make decisions that are most meaningful to them. It would also be difficult to support competence if our client has no interest in mastering a particular skill. Our services will likely not be beneficial.
This can also be viewed with a glass-half-full perspective! If the team can figure out what goal is most meaningful for their client, they can move towards supporting that goal instead. (And since our services are attached to a goal, we can make a decision here whether this new goal requires our services.) And with success towards that meaningful goal, the client may later want to return to work towards the previously-set goal.
Final Notes
To summarize, when deciding needs for services we need to:
-
- Attach your service to a functional goal that is meaningful to the client
- Collect data: times you delivered the service, interventions tried, progress towards the goal, other data such as any change in status
- Use the data to make an informed decision
- Take a glass-half-full view of the data
Of course there may be other reasons to discontinue services. So join the conversation by commenting below. Here at Apply EBP, we do the heavy lifting of presenting the most current evidence, and how you apply them for your clinical reasoning when deciding need for services. Check out these courses:
Feel free to share this article and/or the above video with your school team so that you are all on the same page. Email the YouTube link to them, or use the video when a PD opportunity arises. Cheers!
REFERENCES
-
-
- APTA (2014). Guide to Physical Therapy Practice.
- ASHA’s Admission/Discharge Criteria in Speech-Language Pathology Guidelines
- Boop, C., Cahill, S. M., Davis, C., Dorsey, J., Gibbs, V., Herr, B., … & Lieberman, D. (2020). Occupational therapy practice framework: Domain and process fourth edition. AJOT: American Journal of Occupational Therapy, 74(S2), 1-85.
- Vialu, C., & Doyle, M. (2017). Determining need for school-based physical therapy under IDEA: Commonalities across practice guidelines. Pediatric Physical Therapy, 29(4), 350-355.
-